

Adapting to the challenge
Featured Products Promotional FeaturesPosted by: Dental Design 31st January 2024
Tooth loss can be stressful for patients, with a change to their dentition potentially affecting function and aesthetics, and in turn, their confidence. They may seek a dental implant for a long-lasting, stable restoration, which can restore a natural-looking and feeling smile.
Clinicians may encounter a range of issues – lost anterior teeth, decaying pre-molars – but some of the most difficult cases may involve offering posterior implants.
Patients are demanding modern and streamlined solutions, so it’s important for clinicians to consider how this affects the types of treatments that they offer – and what it means for the equipment and techniques they use.
A modern treatment
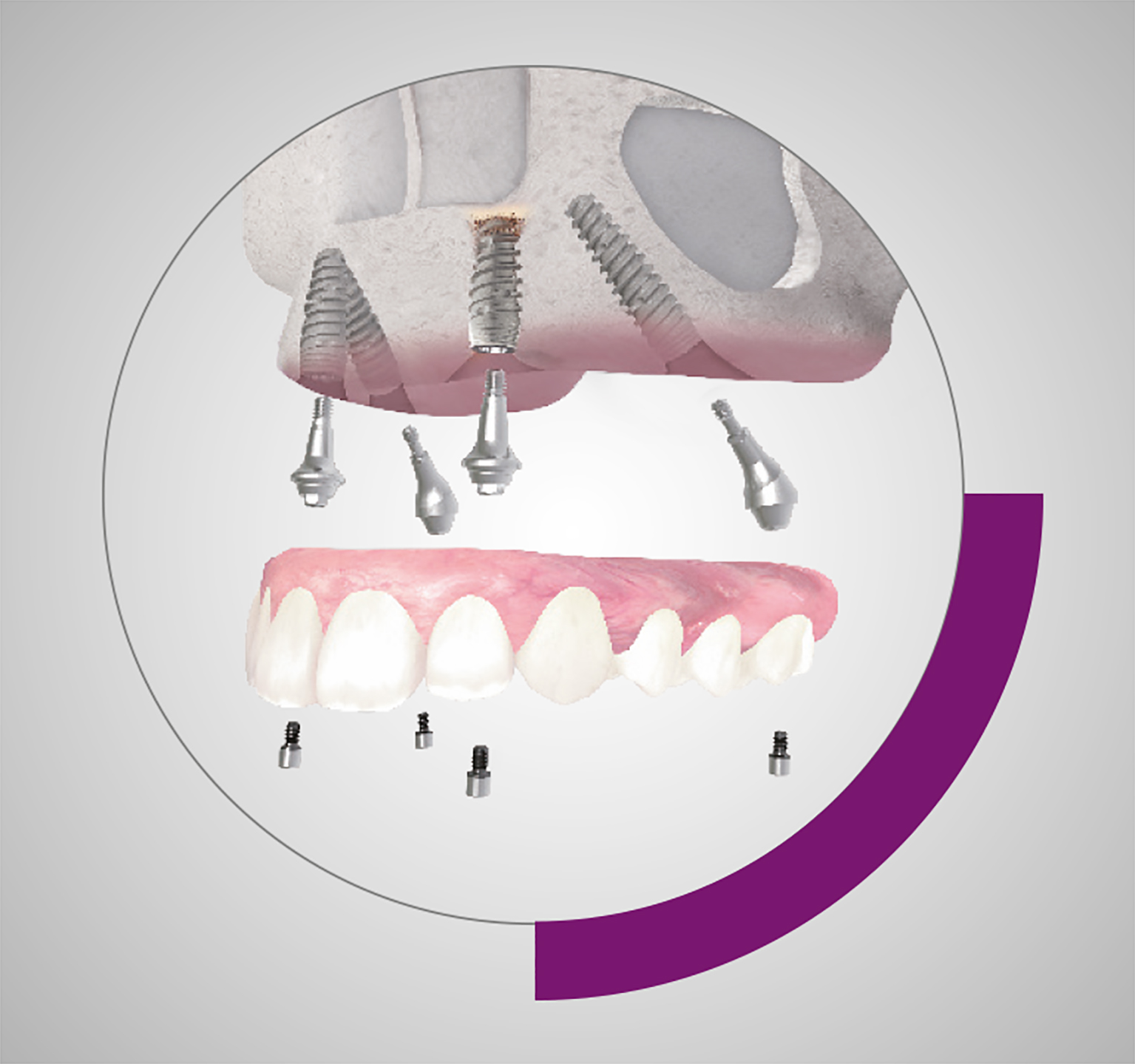
Immediate implant placement is quickly becoming a treatment option preferred by patients. When successfully carried out, an immediately placed implant can restore the dentition with a reduced treatment time, without compromising on aesthetics, function and longevity.
Following the removal of a tooth, the alveolar bone will undergo atrophic change that reduces the available bone volume for implant placement.[i] This can be a functional and aesthetic issue faced when using delayed placement protocols.i In contrast, placing an implant directly after an extraction, particularly in the posterior region, offers a number of benefits for the clinician. Firstly, immediate placement can help to preserve the extraction site, maximising the volume of bone that is available to work with.i
The extraction site may also act as a partial surgical guide. A clinician could follow the extracted roots to ensure that the ideal positioning and orientation of the implant is achieved.[ii]
Immediately placed implants have an equally high survival rate when compared to delayed placement in a molar post-extraction site.[iii] However, to maximise the clinical and aesthetic outcomes of each unique case, clinicians must ensure they are using the appropriate equipment as well as an effective technique.
The difference a component makes
Achieving primary stability, especially in immediate implant placement, is essential to facilitate successful osseointegration in the long term. When a molar is extracted, the fresh socket may have no remaining bone to support the implant and achieve this stability.[iv] However, immediate placement could still take advantage of the limited bone in the surrounding structures. Acting quickly following an extraction could allow a clinician to utilise the nearby bone before atrophy takes place, and use this to attain primary stability.
Clinicians should utilise the widest implant diameter necessary and, where appropriate, consider the use of bone augmentation procedures to provide a sufficient bone density for success.iv A wider implant can offer an improved chance of achieving primary stability by making contact with the walls of the post-extraction socket. The introduction of a biomaterial can help to narrow the alveolar gap, where a wider implant cannot suffice.
In the posterior region, the human bite force is triple that of the anterior:[v] occlusal overload is an important failure factor, so mitigating this power through the implant structure itself must be considered. It has been reported that increasing the implant diameter can reduce the intensity of stresses along its length, as well as lower stress values in the bone.[vi] Increasing the load-bearing capacity is therefore possible with a wider implant, making it an increasingly appropriate option in this region of the mouth.
Bones and all
 Alongside the implant’s relationship with the bone, with stability and occlusal forces considered, a clinician should also think about care for the soft tissue. A healing abutment is generally the option of choice to maximise health and aesthetics.
Alongside the implant’s relationship with the bone, with stability and occlusal forces considered, a clinician should also think about care for the soft tissue. A healing abutment is generally the option of choice to maximise health and aesthetics.
This key component is used to recover or modify the soft tissue following implant placement, for clinical and aesthetic purposes.[vii] Healing abutments may be customised for the individual patient, but wider solutions can generally be used in the posterior, given the size of the implant and the surrounding site. Overall, they are essential in modern dentistry for the control of the soft-tissue emergence profile. [viii]
The ideal outcome is a natural-looking profile that also protects the health of the soft tissue and the underlying bone. A healing abutment does this by preventing the formation of food traps.viii If debris builds up around the implant and soft tissue, a patient could develop peri-implantitis – with potential for implant failure.[ix]
When using the right components, difficult cases in the posterior can become manageable and successful. Neodent®, a Straumann Group brand, offers exceptional posterior solutions within their Grand Morse® range. The Grand Morse® Helix® implants are available with Ø 6.0 mm and Ø 7.0 mm diameters, to maximise primary stability in multi-rooted extraction sockets. Wide healing abutments are also available, for options that provide a natural-looking emergence profile in a healthy site.
Posterior implants place unique demands upon the clinician – less bone in the extraction socket, high occlusal load, aesthetic molar restoration. Immediate implant treatment is more than possible, though, and where appropriate it can restore a patient’s confidence in excellent time.
![]()
For more information, please visit
[i] Hattingh, A., De Bruyn, H., Van Weehaeghe, M., Hommez, G., & Vandeweghe, S. (2020). Contour changes following immediate placement of ultra-wide implants in molar extraction sockets without bone grafting. Journal of clinical medicine, 9(8), 2504.
[ii] Chen, H., Wang, W., & Gu, X. (2021). Three-dimensional alveolar bone assessment of mandibular molars for immediate implant placement: a virtual implant placement study. BMC Oral Health, 21, 1-8.
[iii] Atieh, M. A., Payne, A. G., Duncan, W. J., de Silva, R. K., & Cullinan, M. P. (2010). Immediate placement or immediate restoration/loading of single implants for molar tooth replacement: a systematic review and meta-analysis. The International journal of oral & maxillofacial implants, 25(2), 401.
[iv] Lee, W. (2021). Immediate implant placement in fresh extraction sockets. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 47(1), 57-61.
[v] Flanagan, D. (2017). Bite force and dental implant treatment: A short review. Medical Devices: Evidence and Research, 141-148.
[vi] Bedrossian, E. (2020). Do Dental Implant Width and Length Matter? Compendium of Continuing Education in Dentistry, 41, 7.
[vii] Kyaw, T. T., Abdou, A., Nakata, H., & Pimkhaokham, A. (2022). Dental implant healing abutment decontamination: A systematic review of in vitro studies. Int. J. Oral Implantol, 15, 311-324.
[viii] Bishara, M., Kurtzman, G. M., & Krause, E. S. (2020). Implant restorations: establishing a proper emergence profile. Compendium, 41(8).
[ix] Kochar, S. P., Reche, A., & Paul, P. (2022). The etiology and management of dental implant failure: a review. Cureus, 14(10).





