A straightforward endodontic solution to acute apical periodontitis, completed in a single visit
Featured Products Promotional FeaturesPosted by: Dental Design 27th January 2024

Dr Sagi Shavit graduated from dental school in 2009 in Bucharest and shortly afterwards developed a special interest in endodontics. He undertook a number of endodontic training courses, including microsurgical endodontics, in London and, in 2015, he gained an MSc in Endodontics from the University of Chester. He now treats endodontic patients exclusively at Cleveland Terrace Dental Practice, Darlington.
Here, he presents a case where a patient favoured a treatment plan of endodontic therapy as a solution to her oral pain.
Initial presentation and diagnosis
A female patient in her 50s was referred to our clinic regarding her upper second premolar. She complained of painful episodes and pain upon mastication.
The referring GDP had already accessed and dressed the tooth. A radiographic examination (see figure 1) shows deep restoration on the UL5, with no associated periapical pathology. The root shows a 45-degree curvature in the apical third.
A diagnosis of acute apical periodontitis following pulp necrosis, was placed.
The treatment options of endodontic treatment or extraction of the tooth were discussed. The patient decided to have endodontic treatment, if possible.
Treatment steps
The tooth was accessed under rubber dam (the framed Flexi Dam from COLTENE) and a single canal was located with the aid of the dental operating microscope. A HyFlex™ EDM OneFile (~/25), manufactured by COLTENE, was used for coronal enlargement, up to the curvature which was estimated radiographically at 18mm.
The working length was determined using the CanalPro™ Apex Locator (COLTENE) at 21mm.
A smooth glide path was achieved using manual 8 and 10 K-Files, under copious irrigation of 5.25% sodium hypochlorite.
Mechanical instrumentation continued using the HyFlex™ EDM OneFile (~/25) to the working length. An intra-operatory radiograph (see figure 2) with a gutta-percha point confirms the correct working length. This was performed under copious irrigation of 5.25% sodium hypochlorite, and a final rise with 17% EDTA. Both irrigation solutions were activated ultrasonically using a cordless endodontic activator, the CanalPro™ EndoUltra (COLTENE).
Especially when working in curved canals, it is advisable to inspect the gutta-percha point after it is removed from the canal, to ascertain that there are no deformations, and it is well seated apically (see figure 3).
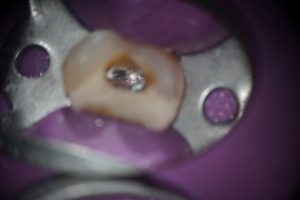
The canal was then dried using matching paper points, and obturated using warm vertical compaction, due to the oval shape of the canal in the coronal third. Figures 4 and 5 show the down pack phase both clinically and radiographically; on Figure 4, the intra-canal view, you can clearly note the oval shape.
The access cavity was sealed with resin composite and the patient was advised to return in three months for outcome assessment of the treatment.
The post-operative radiograph (see figure 6) shows adequate 3-dimensional obturation of the endodontic space.
Conclusion
This case was completed in a single visit, with a single file, quickly and safely, and both myself and the patient were satisfied with the outcome.
COLTENE offers a wide variety of tools that can help clinicians delivering endodontic treatment achieve predictably good results. From the pre-framed Flexi Dam, through to apex locators and endo motors and super-elastic files like the HyFlex™ EDM range, the products allow me to simplify my workflows.
![]()
For more on COLTENE, visit www.coltene.com,
email info.uk@coltene.com or call 0800 254 5115.