

Life-changing treatment for a dental phobic patient
Featured Products Promotional FeaturesPosted by: Dental Design 29th March 2023

A 57-year-old female patient presented to the practice needing to change to her smile and her life. She had become quite depressed about her appearance – she even worked night shifts to avid seeing people. She reported that she was unable to smile around friends or family and that all of this had led to anxiety issues, especially with regards to seeking dental help. It was a big step for her to have even contacted the practice, having not seen a dental professional for 19 years.
Assessment
The most important part of our initial consultation – which was conducted via video call – was to listen to her concerns and really understand the challenges that she was facing. As dentists, we must take on many different roles outside of providing dental treatment and one of these is doing what we can to support our patients’ emotional and mental wellbeing.
We discussed everything she disliked about her smile and anything that she was worried about regarding treatment. I was then able to start explaining how it would all work and what we could do to make every single stage of treatment as comfortable for her as possible.
This was followed up with an in-practice consultation, which served to meet the patient properly, introduce her to the team and build her confidence with being in the dental environment. During this appointment, we also began the clinical assessment (Figures 1-9).
The patient had initially been referred to me by her daughter for Invisalign treatment. She was a regular smoker but was generally fit and well. A CBCT scan was taken to further examine the anatomy and bone health.
The next step was a comprehensive evaluation, including a full set of clinical photographs, intraoral imaging with the iTero scanner, 6-point pocket chart and emphasis of how important smoking cessation would be. A diagnosis was made and discussed with the patient in detail. This included failing upper dentition, generalised, moderate periodontal disease in the lower arch and retained roots of the lower molars.
Treatment planning
The goals of treatment were to motivate and support smoking cessation, stabilise the periodontal condition and replace the failing dentition – all the while helping the patient to reduce her dental anxiety. For the upper arch, the hopeless prognosis of the remaining teeth made extraction the only option, so we considered restorative solutions such as dentures with or without locators, and full arch fixed treatment. The patient expressed a preference for implant placement. For the lower arch, periodontal therapy was again recommended, along with removal of the retained roots and a cobalt chrome prosthesis.
The patient’s smoking habit, active periodontal disease and high smile line were all risk factors for any restorative treatment provided. This was explained to the patient and all the appropriate hygiene support and advice was provided in an easy-to-understand way so that she could retain control and understood her role in her rehabilitation.
Usually, we would have stabilised both the upper and lower arch before providing a restorative solution like implants in either arch. However, due to patient’s extreme anxiety and personal desires, it was decided to treat the upper arch first and then the patient would return for lower stabilisation and restoration. All the potential risks, limitations and benefits of the proposed treatment were explained to the patient in detail to ensure informed consent.
Treatment
Early on in the treatment journey, the patient’s dental anxiety was reduced – she was able to attend with less fear each time and sedation was not needed for any therapies provided. She also very successfully stopped smoking and was committed to her dental journey with no missed appointments and renewed enthusiasm for her health.
Her plaque scores were reduced through regular hygiene support and an improved at-home routine. The periodontal disease was arrested and her conditions stabilised.
Conditions were optimised to increase success with the proposed implant treatment. The CBCT and intraoral images previously taken were used to plan the exact position, angulation and depth of implants, with a prosthetically-driven approach in mind. Six Axiom PX tissue level dental implants (10 x 2.5mm, 12 x 2.5mm, with 2.5mm collars) were placed as per the plan, ensuring clearance for the prosthetic with a ridge reduction procedure. These implants were selected due to the high primary stability they can achieve and the system’s ease of use.
Impression copings were placed and a new impression and bite registration were taken to fabricate the temporary prosthesis, which was designed to scallop the soft tissue sin preparation for final restoration. This was created by Phil Morrison, owner of Morrison Aesthetics Dental Lab in Oxford. The implants were immediately loaded, occlusion checked and the patient given standard post-operative instructions.
Once the try in of the bridge was verified in the surgery, with approval from both patient and clinician, the framework design was returned to Lee Mullins, owner of The Dental Laboratory in Leeds. This was reverse engineered into each individual tooth and sent to Anthogyr/Simeda® for production by way of additive printed titanium, which housed the inLink® straight to fixture components.
Each tooth was then individually cemented to the framework and the gingiva reproduced using a zirconia infused composite. This process ensured exceptional fit, function and aesthetics in the mouth (Figures 11-14).
Outcome and discussion
The patient returned to the practice one week later for a post-operative review of the surgical site and to ensure the soft tissues were healing correctly – no issues were detected (Figures 15-19).
Another few months later and the patient is a completely different person. She reported a life-changing impact thanks to her new teeth, which have restored her self-image and kept her motivated to remain a non-smoker. She can now leave the house with confidence and really enjoy life once again. The patient is also no longer fearful of the dentist, which is something I am particularly proud to have helped.
The next step is periodontal therapy in the lower arch, followed by removal of the remaining teeth with a hopeless prognosis. The patient will return for the fitting of a lower chrome denture once the soft tissue condition has been stabilised.

Figure 1 – pre treatment smile

Figure 2 – pre treatment anterior view

Figure 3 – pre treatment left lateral smile

Figure 4 – pre treatment right lateral smile

Figure 5 – pre treatment anterior retracted

Figure 6 – pre treatment left lateral retracted

Figure 7 – pre treatment right lateral retracted

Figure 8 – pre treatment upper occlusal view

Figure 9 – pre treatment lower occlusal view

Figure 10 – post upper teeth extraction
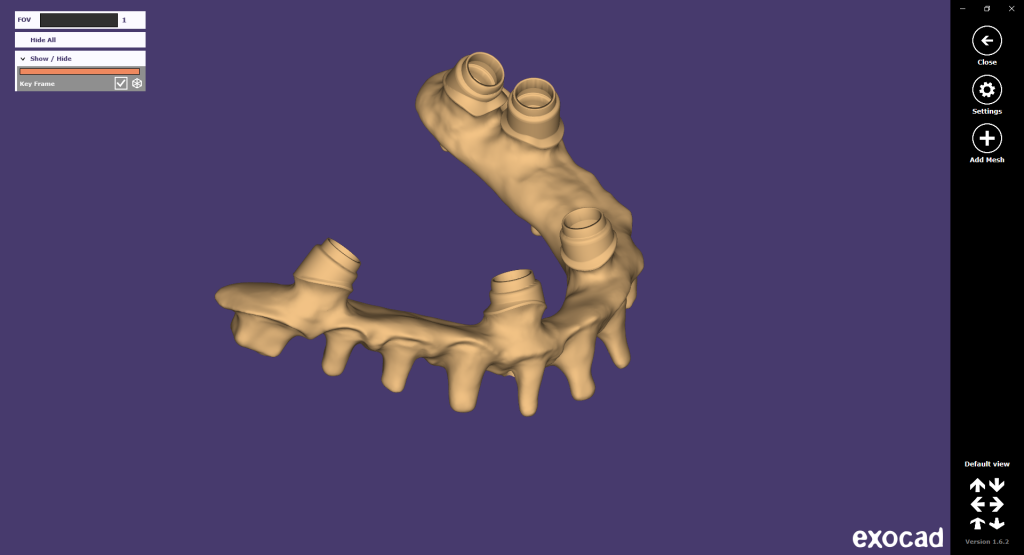
Figure 11 – Prosthetic design process int he lab

Figure 12 – upper prosthesis

Figure 13 – upper prosthesis

Figure 14 – upper prosthesis

Figure 15 – post upper arch implant placement and restoration

Figure 16 – post upper treatment left lateral

Figure 17 – post upper treatment right lateral

Figure 18 – post upper treatment smile

Figure 19 – post upper treatment OPG
For more information about the Anthogyr implant systems available, please visit www.straumann.com
Author:
Dr Sachin Sedani is the Principal Dentist of North Hill Dental in Colchester.





