

Optimise full arch rehabilitation with effective planning
Featured Products Promotional FeaturesPosted by: Dental Design 28th February 2022

Dr Ferhan Ahmed shares a recent case where he provided planning and surgical support to a colleague – Dr Melanie Edwards of West Parade Dental care in Lincoln – for an implant case as part of the training programme he offers.
A female, 67-year-old patient presented seeking an alternative solution to her existing upper denture. She was struggling with movement of the denture while speaking and eating and it was beginning to affect her confidence and ability to communicate with others. She was very conscious of the denture moving around and slipping down, and this was having an increasingly negative impact on her quality of life.
A comprehensive medical history and clinical assessment was conducted. Aside from being a well-controlled asthmatic, the patient was fit and well, with no other health concerns. Her oral hygiene was good and there were no abnormalities detected.
After discussing the patient’s concerns with her, four treatment options were presented:
- No treatment
- A new removable denture
- A removable, implant-retained denture
- A fixed implant-retained prosthesis
The patient was most interested in the fixed solution due to the convenience and peace of mind this would provide.
Treatment planning
A full set of clinical photographs, intraoral scans and a CBCT were deemed appropriate and taken. This information was used to assess the patient’s smile line, lip support requirements and bone availability – including bone height, width and distribution as well as its suitability for multiple implant placement.
It is always important to combine the anatomy and clinical requirements with the patient’s desires to find the most viable solution. As part of the treatment planning process, digital technology can be used to further engage the patient, determining any changes to the tooth shape, length and width for the restorative phase.
All of this information is shared with the dental technician, who provided a restorative guide and interim denture for the day of surgery in this case. Every aspect of treatment was planned virtually, involving both clinicians, the technician and the patient to ensure the best possible result. In the end, the plan was to perform an alveoloplasty and place four dental implants with maximum anterior-posterior spread for same day teeth. A final FP3 prosthesis would ultimately be delivered.
Surgical treatment
Four Neodent Grand Morse Helix dental implants of 4mm x 13mm and 4mm x 11.5mm were placed in the maxilla at the pre-determined positions. I use these as my preferred implant system for full arch immediately loaded cases due to their highly predictable, reproducible results. They enable high primary stability and are simple for clinicians who are new to immediate load full arch implants to develop their skills with, which is why I choose them when training and mentoring.
A full thickness flap was extended from the distal aspect of the second molar on one side to the distal aspect of the second molar on the other side. This was done with respect for the anatomical landmarks identified, the nasal floor, maxillary sinus bulbosities, nasopalatine canal and the palatal shelf.
An alveoloplasty was carried out, as determined in the planning. This bone reduction is important for restorative success – adequate restorative space must be created for the final restoration in order to deliver the most functional and aesthetic results for the patient. In this case, we planned for a FP3 metal acrylic final restoration.
The patient left the practice on the day of surgery with her fixed interim bridge in place. Once healing has occurred and the patient has had time to become accustomed to the interim bridge, a definitive prosthesis will be fabricated.
Review
Full arch rehabilitation is an advanced implant procedure, so it’s important to have a mentor when you first enter the field. Whether a colleague offers a second opinion and support virtually or is by your side during surgery will vary according to your clinical experience and confidence.
Even full arch implants can be made simpler with innovative products and careful planning – as demonstrated by this presentation. Case selection is really important for the best result, especially when starting out with this type of treatment modality. It is just as crucial to really understand the patient’s psychology and desires for treatment. As clinicians, we need to deliver solutions to the patient’s concerns, meeting their aspirations as well as the clinical requirements of their anatomy.
Treatment planning is integral for this. Everything will work on the day of surgery if the planning is appropriate. This means that the clinician(s), technician and patient must align their aspirations and expectations so they work towards a common goal. This allows a streamlined surgical process and more predictable results. When you can reproduce high quality outcomes day in day out, it also gives patients confidence in your skills and your team.
For more information, please visit https: www.neodent-uk.co/efficiency

About the author:
Dr Ferhan Ahmed is dual-qualified in dentistry and medicine. His current practice is limited to dental implants and surgical dentistry. He qualified from the University of Glasgow (UK) with a BDS in 2005 and from the University of Liverpool (UK) with an MBChB in 2012. Since completion of vocational training, he has exclusively focused training and research in the area of oral and maxillofacial surgery. Dr Ahmed is involved in teaching and mentoring within the field of dental implants and surgical dentistry. His practice in dental implants involves conventional implants, complex bone grafting and extra maxillary implants such as pterygoids and zygomatics.
Images:

Fig 1

Fig 2

Fig 3

Fig 4

Fig 5
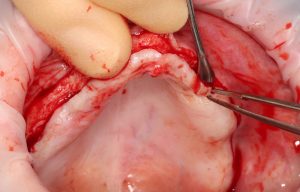
Fig 6 -surgical phase incision and flap reflection
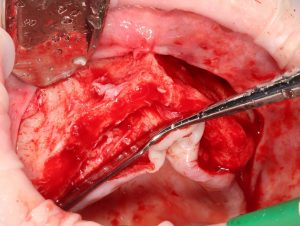
Fig 7 -exposure of the alveolar ridge illustrating ridge reduction right side

Fig 8 -exposure of the alveolar ridge illustrating ridge reduction right side

Fig 9 -prothetic guide in place

Fig 10 -Multiunit healing cap in place

Fig 11 – Wound closure

Fig 12

Fig 13

Fig 14

Fig 15

Fig 16-post-operative smile shot with temp-restoration in

Fig 17

Fig 18

Fig 19

Fig 20 -final prosthesis in left lateral view

FIg 21 -final prosthesis in right lateral view

Fig 22 -final prosthesis in occlusal view

Fig 23





