

Aesthetic periodontics – the potential of surgical crown lengthening
Featured Products Promotional FeaturesPosted by: Dental Design 26th October 2021

When approaching periodontology, we often think about the health of the gingiva and the treatment or management of disease. While this is the priority, it is also often necessary to consider aesthetics too. The soft tissue is integral to the appearance and function of the teeth, so optimising every aspect of it is beneficial in achieving the best possible outcomes for patients.
Soft tissue impact on treatment
The soft tissue fulfils several roles within the mouth, including protection of the tooth roots and/or dental implants, prevention of infection and improving smile aesthetics.
When assessing the gingiva either visually or with a periodontal probe, it is commonly characterised according to its biotype. Typically, it is referred to as ‘thick’ or ‘thin’ – more specifically ‘scalloped and thin’ or ‘flat and thick’ – which relate to gingival thicknesses of ≥1 mm or <1.0mm respectively.[i]
It has been proposed that gingival biotype is one of the main factors influencing the success of root coverage procedures or restorative dental treatments. Patients with a thinner gingiva are more likely to experience recession following non-surgical periodontal therapy and mucogingival problems as a result of orthodontic treatment.[ii] Tissue biotype can also affect site preparation and surgical outcomes with regards to dental implant planning and placement.[iii] All of these have the potential to impact final aesthetics, so careful consideration should be given to minimising potential soft tissue complications when working with thinner biotypes.
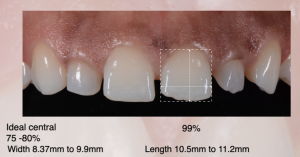
However, tissue thickness is not the only aspect to think about – the position of the gingiva in relation to the teeth and smile line is also important. We would typically categorise a ‘high’, ‘average’ or ‘low’ smile line, which is generally determined by how much cervico-incisal length of the maxillary anterior teeth and adjoining gingiva is visible when smiling. A high smile line reveals the entire length of the teeth with a band of the adjoining gingiva, an average smile line 75-100% of the teeth with interproximal gingiva and a low smile line less than 75% of the anterior teeth with no gingiva visible.[iv] Though not an exact science, there is evidence to suggest that high smile lines (or ‘gummy smiles’) are generally perceived to be less aesthetic. [v]
Crown lengthening indications and contra-indications
According to the American Academy of Periodontology,[vi] crown lengthening is “a surgical procedure designed to increase the extent of supragingival tooth structure, primarily for restorative purposes, by apically positioning the gingival margins with or without the removal of supporting bone”. Indications for treatment include:[vii]
- Restorative needs
- To increase clinical crown height lost due to caries, fracture or wear
- To access subgingival caries
- To produce a ‘ferrule’ for the provision of a post crown
- To access a perforation in the coronal third of the root
- To relocate the margin of restorations that are impinging on biological width
- Aesthetics
- Short teeth
- Uneven gingival contour
- Gummy smile
Contra-indications include:
- Inadequate crown-to-root ratio
- Non restorable caries or root fracture
- Aesthetic compromise
- High furcation
- Inadequate predictability
- Tooth arch relationship inadequacy
- Compromising of adjacent periodontium or aesthetics
- Insufficient restorative space
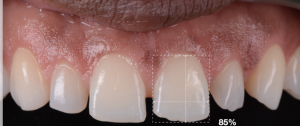
Essentially, crown lengthening can be utilised to improve smile aesthetics by increasing the amount of tooth length visible and reducing the amount of gingiva in the smile line. The most important consideration is to ensure that surgery doesn’t make the appearance of the teeth and gums worse – the crown-to-root ratio is a crucial aspect of the treatment planning process!
Another vital factor to asses and plan for is the biological width – which is the dimension of soft tissue that is attached to the part of the tooth that is coronal to the crest of the alveolar bone. This is important for periodontal health and poor management of the biological width during any treatment, including crown lengthening, can result in increased risk of periodontitis. Other possible signs of biological width violation are chronic progressive gingival inflammation, bleeding on probing, localised gingival hyperplasia, clinical attachment loss and alveolar bone loss.[viii] For a thin biotype, there is also an increased risk of gingival recession and bone resorption, while a thick biotype is associated with vertical osseous defects around the tooth and pocket formation.
Planning for success
For all these reasons and more, pre-surgical evaluation for crown lengthening must consider periodontal health and gingival biotype, root anatomy, crown-to-root ratio, the presence of caries and endodontic prognosis. This requires radiographic assessment and bone sounding to ensure that the bone is of sufficient height, width and density to facilitate the change in gingival volume. This involves taking a 1mm probe and pushing down from the gingival margin as far as it goes under local anaesthetic.
Of course, this is just the beginning of successful crown lengthening treatment for the aesthetic improvement of patients’ smiles. The Surgical Crown Lengthening Hands-on course with BPI Dental & Education is a great option for any clinicians looking to significantly develop their knowledge and skills in the field. The comprehensive training covers everything discussed here and more, including the surgical procedures themselves, which we will look at in more detail in the next article.
Images





Dr Boota Singh Ubhi
Speciality: Specialist Periodontist & Implant Surgeon
Qualifications: 1992 University of Liverpool BDS, FDS RCS (Edinburgh) MDentSci (Liverpool) MRD RCS (England)
About Me: Leading a select team of experts, Boota has a reputation for routinely surpassing patients’ expectations.
For more details or to book your place on the next Surgical Crown Lengthening course with Dr Boota Singh Ubhi, please visit https://bpieducation.co.uk/dental-courses/surgical-crown-lengthening/
[i] Kan JYK, Morimoto T, Runcharassaeng K, Roe P. Gingival biotype assessment in the esthetic zone: Visual versus direct measurement. The International journal of periodontics & restorative dentistry. June 2010. 30(3); 237-43.
[ii] Manjunath RG, Rana A, Sarkar A. Gingival Biotype Assessment in a Healthy Periodontium: Transgingival Probing Method. J Clin Diagn Res. 2015;9(5):ZC66-ZC69. doi:10.7860/JCDR/2015/13759.5956
[iii] Kao RT, Fagan MC, Conte GJ. Thick vs. thin gingival biotypes: a key determinant in treatment planning for dental implants. J Calif Dent Assoc. 2008 Mar;36(3):193-8. PMID: 18444430.
[iv] Al-Juboori MJ, Al0Juboori AJ, Wan TM, Ting J, Chui LS, Hoe TM, Al-Wakeel HA. The relationship between the lip length and smile line in a Malaysian population: A cross-sectional study. Dental, Oral and Craniofacial Research. 2017. 3(4); 1-5. doi: 10.15761/DOCR.1000208
[v] Sybaite J, Sharma P, Fine P, Blizard R, Leung A. The Influence of Varying Gingival Display of Maxillary Anterior Teeth on the Perceptions of Smile Aesthetics. J Dent. 2020 Dec;103:103504. doi: 10.1016/j.jdent.2020.103504. Epub 2020 Oct 28. PMID: 33129999.
[vi] AAP Connect. Crown Lengthening. Glossary of Periodontal Terms. American Academy of Periodontology. https://members.perio.org/libraries/glossary?ssopc=1 [Accessed August 2021]
[vii] Camargo PM, Melnick PR, Camargo LM. Clinical Crown Lengthening in Esthetic Zone. C D A Journal 2007;3 5,Number7:487-498
[viii] Nugala B, Kumar BS, Sahitya S, Krishna PM. Biologic width and its importance in periodontal and restorative dentistry. J Conserv Dent. 2012;15(1):12-17. doi:10.4103/0972-0707.92599





