









Endodontic treatment is normally categorised into three types. These are: vital pulp therapy (VPT), which aims to maintain pulp vitality; root canal treatment (RCT), which aims to address inflamed/infected pulp and peri-radicular tissues or manage the sequalae of failed previous treatments; and surgical treatment, including apicectomy.
Root canal treatment
It is widely accepted that ‘successful’ RCT is the outcome whereby the patient is asymptomatic, and radiographically healed.[i] However, epidemiologists report a lack of Patient Reported Outcome Measures (PROMs) in endodontic research.[ii] Most patients consider treatment success to be their tooth being saved and pain free – often called a ‘favourable survival outcome’.[iii] Patients may know that their endodontic infection caused bone loss around the tooth, and their dentist aimed to treat the tooth to heal it. Whilst there are exceptions to this, often, patients are unaware or have forgotten about it at future appointments.

Fig. 1 Pre-operative radiograph

Fig. 2 One year review showing bony healing
Research suggests that most RCTs are carried out by non-endodontists, however, they may experience lower success rates than endodontists.[iv] Despite this we tell patients with complex cases, You have an endodontic problem, which I can treat, although I don’t think I will have a success rate as high as a specialist. Also I think the ‘success’ I am discussing is different to what you consider success! What a dilemma! Not something that is easy to navigate, but important to bear in mind.

Fig. 3 Pre-operative radiograph

Fig. 4 Six month follow up review incomplete healing
Factors impacting success rates
The research tells us that, globally, RCT has an overall success rate of 75-85%.[v] There are some factors that affect this outcome more than others. Some are out of our control, such as a patient presenting with:
- Pre-operative lesion associated with their necrotic infected pulp
- A large lesion
- A sinus tract
- Previously root treated tooth

Fig. 5 Large lesion
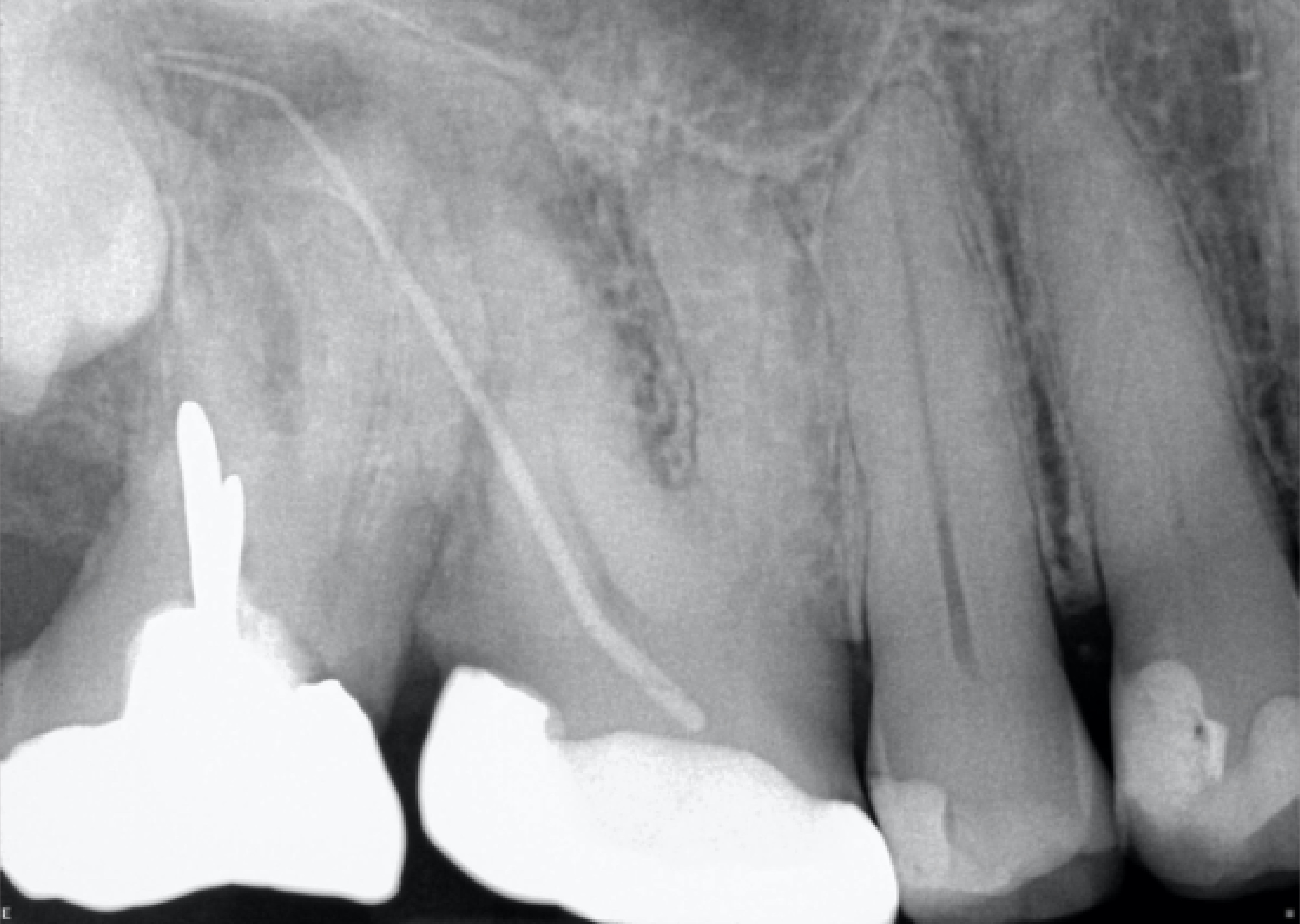
Fig. 6 Previously treated with sinus tract
The majority of the other factors can be controlled and, based upon these, the following recommendations can be made. Ultimately, they are related to the use of aseptic technique and attention to detail during RCT. If we had to change anything in our daily practice to make a big difference, we would start with:
- Use of rubber dam and disinfection of gloves.
- Use of an apex locator to aid prepare and fill the root canal to correct length while maintaining patency.
- Filling the root canal system densely.
- Placing a good coronal seal as soon as possible, and even using an anti-bacterial sub-seal above the gutta percha.
- Placing a cuspal coverage restoration for posterior teeth within the first few months.
These may already be part of your clinical practice, but there are potential challenges and opportunities when it comes to technical and clinical developments and their implementation. The current surge in use of single cone obturation with new (Bioceramic) hydraulic cement sealers is matter of heated debate. There is concern they allow for faster obturation at the expense of demise of core principles of endodontics.[vi] Concern is raised regarding the solubility of these sealers and how, in the long run, they may dissolve in cases of single cone, thus diminishing the initial obturation result. These questions need to be answered before we make significant changes to our workflows.
Vital pulp therapy
We are, however, entering a new era of endodontics, in the form of vital pulp therapy (VPT). The aim of VPT is to maintain the vitality of the dental pulp and involves the removal of infected or damaged pulp tissue. This procedure can be seen as a proactive approach to prevent the need for RCT. Clinical success can mean an asymptomatic tooth which has maintained its vitality in the radicular pulp. Success rates of over 95% have been described, albeit some over relatively short periods.[vii] This form of treatment has now been adopted in teaching institutes, including hands-on sessions for undergraduates and dentists alike.
The British Endodontic Society has promotion, education and advancement of endodontics at its heart. The recently published and freely available “A Guide to Good Endodontic Practice” aims to guide dentists through the concepts discussed above.
Endodontic treatments can be successful whichever type we provide. Let’s consider one last thing in light of the most recent advances. If we take the scenario of 1000 teeth that historically went straight to RCT, at an 80% success rate, 200 would have failed and in some practices that could mean 200 extractions. In contrast, if we treat 1000 teeth with VPT, at a 95% success rate only 50 teeth will fail. If those 50 teeth then go on to have RCT, based on an 80% success rate, 10 fail and extracted. Therefore, if we don’t carry out retreatment or apical surgery, we will have lost only 10 out of the 1000 teeth we started with! Those odds seem pretty good!

Fig. 7 Pre-operative

Fig. 8 Post-treatment VPT
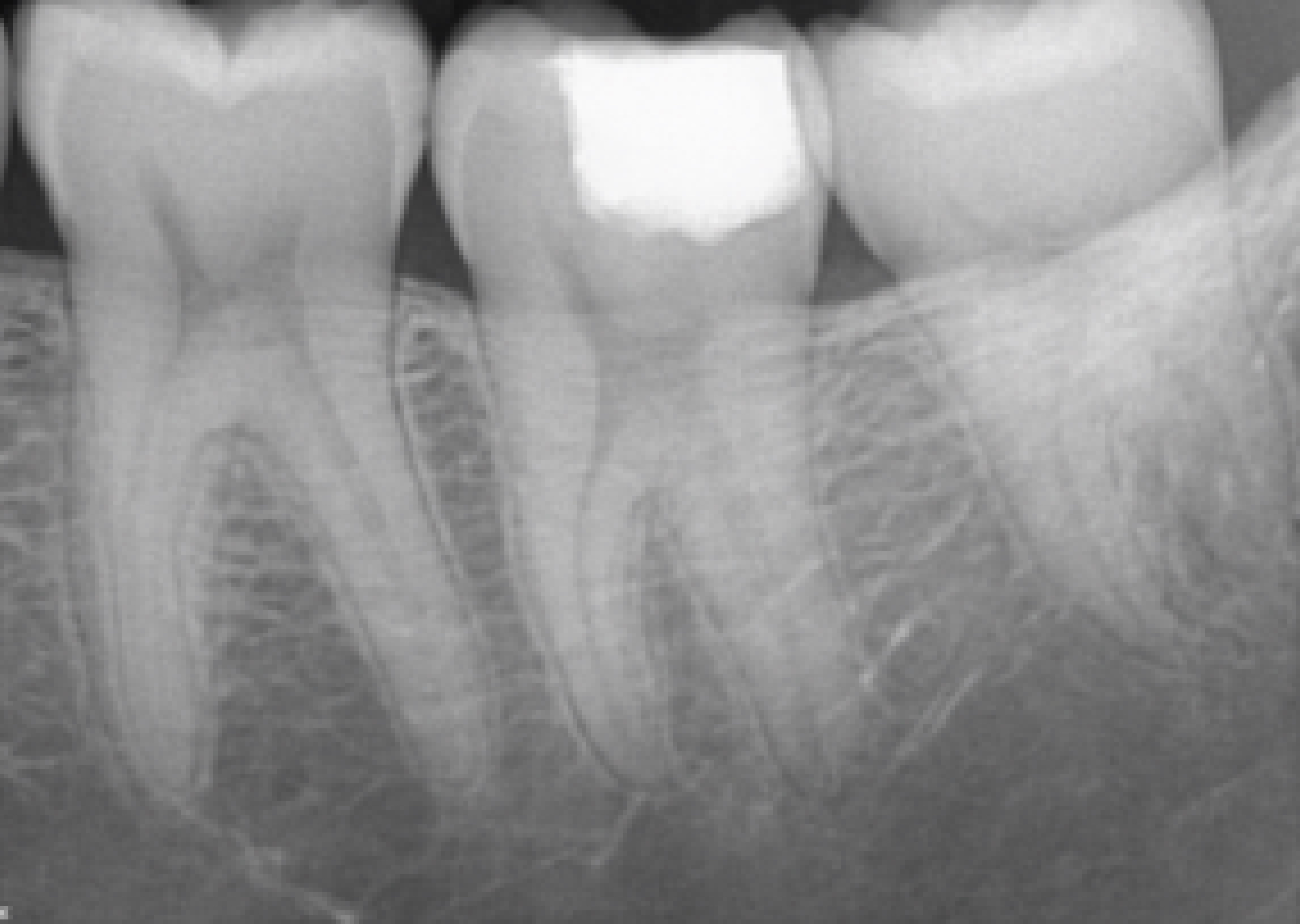
Fig. 9 One year review
This highlights, in very basic terms, that for teeth with vital pulp it is imperative we consider the option of VPT before RCT in suitable cases. RCT remains a good option, and we should consider developing our skills based on the five recommendations above.
Register today for IFEA WEC 2024 at ifea2024glasgow.com/registration
For more information about the BES, or to join, please visit the website www.britishendodonticsociety.org.uk or call 07762945847
Download “A Guide to Good Endodontic Practice” here
Author Bio:
Maria Lessani
BDS MFDS RCPS MClinDent MRD RCS
Specialist in Endodontics
Past President of the British Endodontic Society
Part time Clinical Lecturer at Eastman Dental Institute and Hospital
Practice Partner at Endoclinic, North London.
Maria qualified from Birmingham Dental School in 1996, following which she worked as a Vocational Trainee in an NHS practice in East London. Maria won an award as VT of the year in 1997. In 1998 Maria started a two-year full-time MClinDent (Endodontology) program at the Eastman Dental Institute. Maria gained the MFDS (TC White Medal) from Glasgow. Her name has been included on the GDC Endodontics specialist list since 2002. Currently Maria’s time is divided between endodontic practice, teaching and work with the BES. She is the past president of the BES 2022-3. She has taught undergraduates and continues to teach postgraduates at Eastman Dental Hospital (UCL). She has been involved in original research in relation to Endodontic Outcome in the NHS and contributed to book chapters.
[i] Gulabivala K, Ng YL. Factors that affect the outcomes of root canal treatment and retreatment-A reframing of the principles. Int Endod J. 2023 Mar;56 Suppl 2:82-115. doi: 10.1111/iej.13897. Epub 2023 Feb 10. PMID: 36710532.
[ii] Duncan HF, Nagendrababu V, El-Karim I, Dummer PMH. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology S3-level clinical practice guidelines: A consensus-based development. Int Endod J. 2021 Dec;54(12):2184-2194. doi: 10.1111/iej.13627. Epub 2021 Sep 22. PMID: 34553383.
[iii] Friedman S, Mor C. The success of endodontic therapy–healing and functionality. J Calif Dent Assoc. 2004 Jun;32(6):493-503. PMID: 15344440.
[iv] Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature – part 1. Effects of study characteristics on probability of success. Int Endod J. 2007 Dec;40(12):921-39. doi: 10.1111/j.1365-2591.2007.01322.x. Epub 2007 Oct 10. PMID: 17931389.
[v] Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011 Jul;44(7):583-609. doi: 10.1111/j.1365-2591.2011.01872.x. Epub 2011 Mar 2. PMID: 21366626.
[vi] Cardinali F, Camilleri J. A critical review of the material properties guiding the clinician’s choice of root canal sealers. Clin Oral Investig. 2023 Aug;27(8):4147-4155. doi: 10.1007/s00784-023-05140-w. Epub 2023 Jul 17. PMID: 37460901; PMCID: PMC10415471.
[vii] Kahler B, Taha NA, Lu J, Saoud TM. Vital pulp therapy for permanent teeth with diagnosis of irreversible pulpitis: biological basis and outcome. Aust Dent J. 2023 Jun;68 Suppl 1:S110-S122. doi: 10.1111/adj.12997. Epub 2023 Nov 20. PMID: 37986231.


