


Missing teeth? Easy, put in some implants
Featured Products Promotional FeaturesPosted by: Dental Design 27th February 2023
Dr Chris Leech, Scientific Director for the British Academy of Cosmetic Dentistry (BACD), presents an interesting case example that is often seen in general dentistry. He shows how comprehensive general dental skills– which are firmly advocated by the BACD among all members – are essential to providing a sufficient solution for the patient…
Implants are a fantastic tool we may utilise when restoring a patient’s dentition. However, as with all treatments they need proper planning and diagnostics in order to be successful. If a tooth has failed we must always start with “why”, and then ascertain how we can address the issue. The case below is all too familiar with what I routinely see. Seemingly it often happens in practices where an implantologist comes in and works on referral. They are tasked to “simply” replace missing teeth, often only surgically, and then the usual dentist pops some teeth on top, easy! The importance of managing the patient’s entire dental health can not be emphasised enough and I often find that patients ideally need pre restorative work to their remaining dentition before utilising implant therapy if we want to minimise risk and maximise longevity.
(Presenting Condition – Figures 1a-1c)
The patient had recently moved to the area and so was unable to visit her treating practice. She was having issues in that her implant teeth kept falling off. They had been re-cemented multiple times but the same thing kept happening. She claims she had been reassured this was normal. The radiographs (Figures 2a-2c) revealed severe bone loss around the implants. The patient was informed of our findings and was understandably not happy. At first, she was not entirely accepting of our diagnosis, especially when we explained that we felt the implants would need to be removed or in fact may simply fall out by themselves – most likely those around the lower left bridge. We explained how we felt there was complete occlusal failure occurring and that a full mouth rehabilitation was required.
The patient didn’t sign up to any care with ourselves but then returned around a month later with something in her hand. (Figure 3)
At this point the patient cited how we had informed her that this would likely happen and so now she wished to hear our proposal to restore her mouth to health. The patient also indicated that she would not accept any more implant treatment due to the cost and would prefer a denture.
The first thing we did was remove all the failing implants as well as embarking on some oral hygiene instruction and maintenance with our hygiene team. We also placed some simple composite restorations on the upper centrals to seal over the ominous fracture in the 11 and seal some of the exposed dentine on the palatial surfaces. Our diagnosis was one of an overclosed bite and a restricted envelope of function. The patient did not want a temporary healing denture.
Figures 4a-4c show the result after this initial stage and healing.
Now we had a healthy mouth we could begin to plan the patient’s new vertical dimension and occlusal scheme.
Thanks goes to Ashley Byrne and his team at Byrnes Dental Laboratory for their assistance with this case. Figures 5a-5b
The new vertical dimension and occlusal setup was designed as well as a wax try in for the missing teeth. Data from 3Shape Trios scans of the mouth were used to do this. Direct composite was used on the lower anterior teeth following the model’s proposed redesign using templates. The upper teeth as well as 46 were prepared for crowns with rest seats and guide plans for precision fit cobalt chrome dentures. These teeth were prepared and temporised with Protemp from the models at this stage. As figures 6a-6c below show, we had opened the vertical dimension and addressed the restricted envelope of function. This was “dialled in” directly in the patient’s mouth and we actually opened the vertical dimension more by adding composite to the palatal aspects of the upper centrals using the patient’s profile and passive lip position to guide us to the correct vertical position. A new Trios scan was then taken to communicate this adjustment to the lab.
The crowns were delivered with printed resin try ins of the framework design so that we could check for accuracy. The fit was perfect (it always is from Byrnes). Once this was confirmed the lab was given the go ahead to manufacture the final dentures. Figures 7a-7c
The lab work was returned – figures 8a-8b.
The fit and retention that can be achieved utilising precision preparation of the crowns is very impressive and the patient was delighted. Figures 9a-9c
Of course, the patient has been instructed of the importance of maintaining her oral hygiene and the need for ongoing professional maintenance. Overall, this case was interesting since the failure of the implants was likely not down solely to the implants themselves. The overall demise of the patient’s dentition and traumatic occlusion demonstrated by the amount of tooth wear as well as the repeated debonding of the indirect restorations was the key element to be managed here.
Dr Christopher Leech BDS MAGDS RCS (Ed)
MFDS RCPS (Glasg) Dip Imp Dent RCS (Ed)
After studying Dentistry at Newcastle University Chris also trained at Sheffield University where he discovered a love for dental implants. He has travelled Internationally training to the highest standards and is the Scientific Director for the British Academy of Cosmetic Dentistry. He is also the first dentist in the UK to pass the Membership for Advanced General Dental Surgery with the Royal College of Surgeons Edinburgh and is a member of the Dental Faculty for the Royal College of Physicians and Surgeons of Glasgow. Chris has also been awarded his Diploma in Implantology from the Royal College of Surgeons Edinburgh. He is an examiner for the Royal College and also a member of the Society for the Advancement of Anaesthesia in Dentistry.

Figure 1a

Figure 1b

Figure 1c

Figure 2a
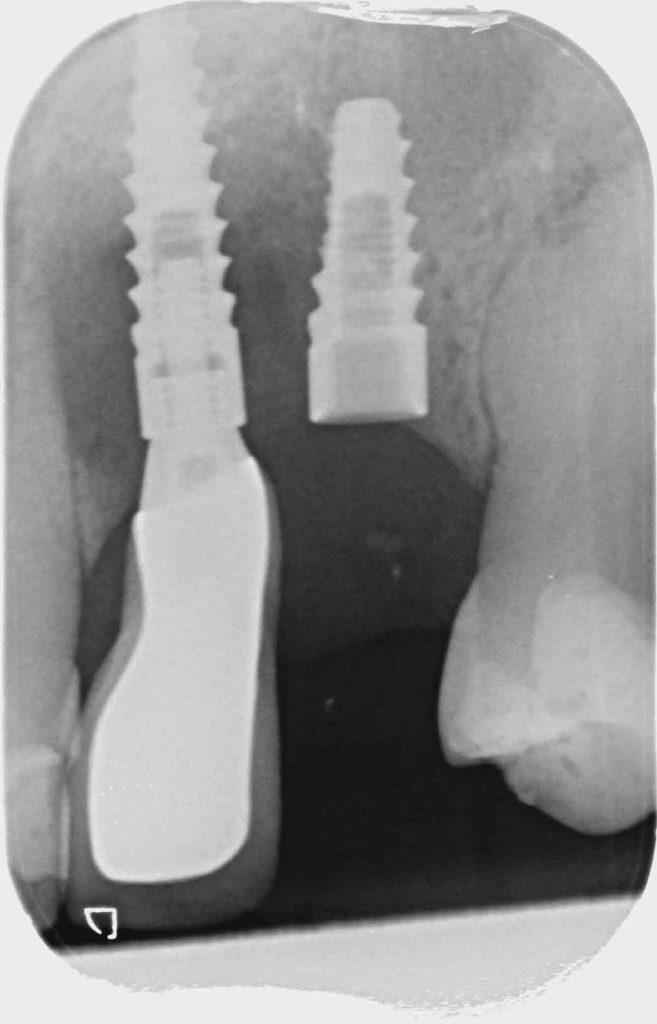
Figure 2b
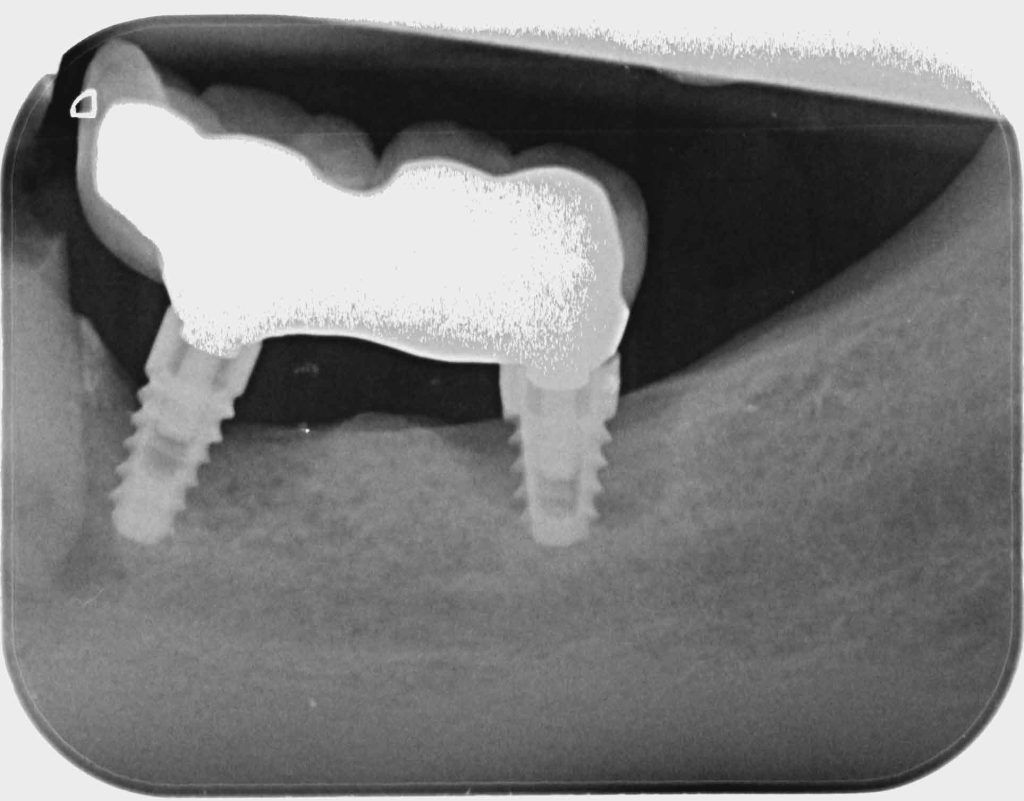
Figure 2c

Figure 3

Figure 4a

Figure 4b

Figure 4c

Figure 5a

Figure 5b

Figure 6a

Figure 6b

Figure 6c
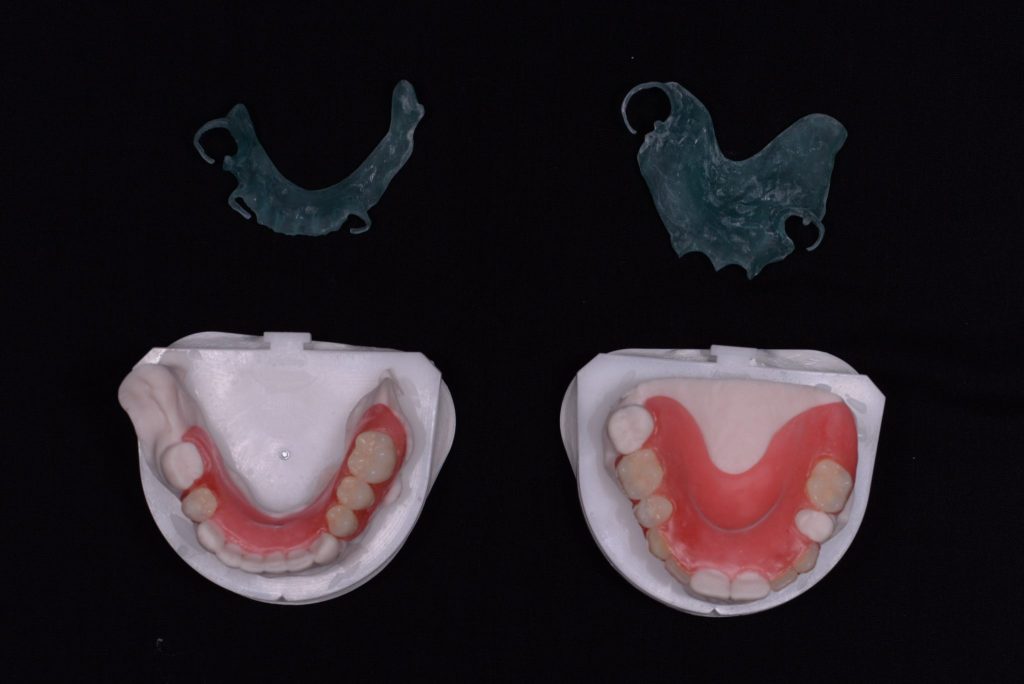
Figure 7a
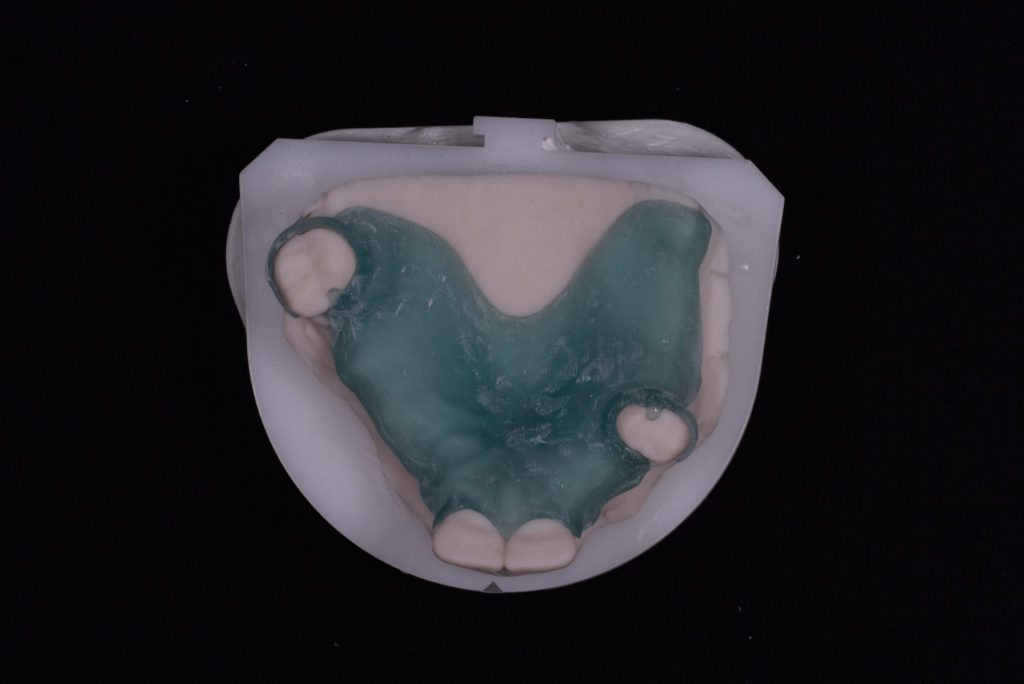
Figure 7b

Figure 7c

Figure 8a

Figure 8b

Figure 9a

Figure 9b

Figure 9c






