


Crown Lengthening Surgery
Promotional FeaturesPosted by: Dental Design 4th May 2021

Periodontal surgery is not limited to the treatment of periodontitis but includes procedures that can be part of a wider restorative plan.
Broadly speaking, we can encounter two different scenarios requiring crown lengthening techniques.
- Functional: in cases of subgingival caries, coronal perforations, fractures, cervical root resorption or tooth wear.
- Aesthetic: excessive gingival display and/or discrepant gingival margins or altered passive eruption.
A correct clinical assessment and a tailored approach based on the patient’s morphotype and site characteristics are all fundamental for a successful outcome.
Where aesthetics are the primary outcome, a diagnostic wax up should be agreed with the patient. This also allows the fabrication of a surgical template to use as a guide during the procedure.
Irrespective of the desired outcome (aesthetics or functional) crown lengthening is performed in line with the guiding principles of the ‘biologic width’. This requires a distance of 4 mm from the osseous crest to the proposed restoration margin or the new gingival margin.
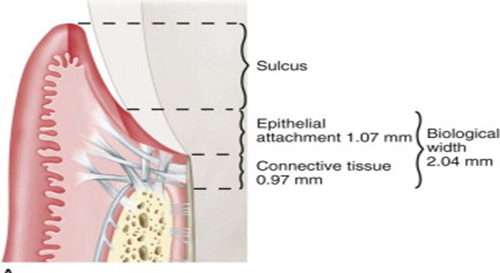
Biologic width. In the new classification (2017), ‘biologic width’ has been renamed the Supracrestal Tissue Attachment & is defined as the ‘cumulative apical–coronal dimensions of the junctional epithelium and supracrestal connective tissue attachment’
Contraindications of crown lengthening surgery include
- Teeth with existing poor crown-root ratios or expected following surgery
- Where removal of bone risks exposure of the furcation (Herrero et al 1995, Lanning et al 2003, Pontoriero & Carnevale 2001)
- Teeth with poor periodontal, endodontic or restorative prognoses
Even though the end goal is the same, there are different ways to lengthen the crown
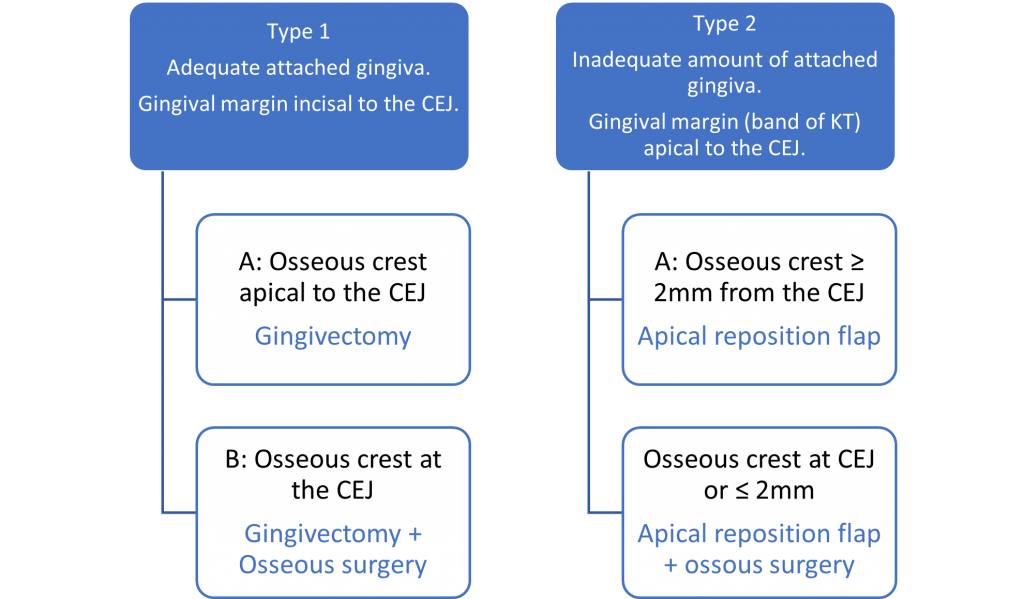
- In cases when there is a wide band of keratinised gingiva, additional crown height can be achieved by gingivectomy with or without osseous surgery.
– External bevel gingivectomy is indicated where osseous resection is not required. To note: in cases of gingival pigmentation, external bevel gingivectomy will produce pink gingival tissue upon initial healing. It is important to consider the patient’s desire to maintain or lessen the existing pigmentation when working in the aesthetic zone. Any alteration will need to match the contralateral gingival pigmentation.
– Internal bevel gingivectomy. This is the most common method of crown lengthening surgery and includes resection of the excess gingival tissue and osseous reduction. It can be indicated for single tooth crown lengthening where uneven gingival contours exists or for multiple teeth. - Where inadequate remaining keratinised gingivae exits, apical repositioning of the soft tissues is completed with or without ostectomy. and is indicated on multiple teeth of the same quadrant or sextant. It is contraindicated in single tooth procedures.
In specific cases of altered passive eruption, two factors have to be considered for the appropriate approach, (Coslet et al 1977):
Orthodontics. An alternative non-surgical/orthodontic approach is forced tooth eruption. This is used also to level and align teeth to achieve aesthetic harmony. Forced tooth eruption with fiberotomy is indicated when the aim is to maintain the gingival margin of the adjacent teeth intact. The action of cutting the insertion fibres every 7-10 days prevents the gingival margin from following the tooth being extruded (Pontoriero et al 1987). This technique is contraindicated in the presence of intrabody defects.
Instrumentation. Bone removal can achieved with conventional surgical burs – tungsten carbide or diamond coated burs; piezoelectric tips or specific lasers. Skilled soft tissue handling using a minimally invasive approach aims to reduce post-operative discomfort and reduce healing time. In aesthetic cases, management of the papilla is critical to prevent post-surgical loss and the development of ‘black holes’
When to restore? Soft tissue rebound has been investigated in detail. In 33% of the cases, coronal shift of 1-3 mm occurred, while in others (29%), 1-4 mm of recession was observed, over a period of six weeks to six months (Brägger et al 1992). Thick phenotypes showed a higher tendency of rebound, up to 12 months after surgery (Pontoriero & Carnevale 2001).

The decision therefore to wait 3 months or 6 months to restore will be determined by the nature of the case – functional or aesthetic – and the thickness of the remaining attached gingivae.
Want to learn to perform these surgcical procedures ? Join us in Florence: https://online.fliphtml5.com/hgfxm/iarj/
About the authors

Dr Ros O’Leary
Ros has been on the GDC specialist list since its inception in 1999, limiting her clinical practice to periodontics for over 20 years. She is highly experienced in the treatment of gum disease and understands that patient involvement in the process of periodontal care is the key to success.

Dr Estela Baz
Having received her Periodontics MClinDent from Eastman Dental Institute, Estela now works at the Perio & Implant DRC, limiting her scope of practice to Implants & Periodontics.
References
Brägger, U., Lauchenauer, D. and Lang, N.P. (1992), Surgical lengthening of the clinical crown. Journal of Clinical Periodontology, 19: 58-63. https://doi.org/10.1111/j.1600-051X.1992.tb01150.x
Coslet JG, Vanarsdall R, Weisgold A. (1977) Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan. ;70(3):24-8. PMID: 276255.
Herrero F, Scott JB, Maropis PS, Yukna RA. (1995) Clinical comparison of desired versus actual amount of surgical crown lengthening. J Periodontol. ;66(7):568-71. doi: 10.1902/jop.1995.66.7.568. PMID: 7562348.
Lanning SK, Waldrop TC, Gunsolley JC, Maynard JG. (2003) Surgical crown lengthening: evaluation of the biological width. J Periodontol. 74(4):468-74. doi: 10.1902/jop.2003.74.4.468. PMID: 12747451.
Pontoriero R, Carnevale G. (2001) Surgical crown lengthening: a 12-month clinical wound healing study. J Periodontol. 72(7):841-8. doi: 10.1902/jop.2001.72.7.841. PMID: 11495130.
Pontoriero, R & FJ, Celenza & Ricci, G & Carnevale, Gianfranco. (1987). Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. The International journal of periodontics & restorative dentistry. 7. 30-43






