


When narrow canals present the risk of file fracture: careful file selection for endodontic success – Dr Peter Nixon
Featured Products Promotional FeaturesPosted by: Dental Design 1st August 2019

 Peter Nixon has been a hospital consultant and specialist dentist for over
Peter Nixon has been a hospital consultant and specialist dentist for over
10 years, working for the Leeds Teaching Hospitals as well as in specialist private practice. His areas of speciality are restorative dentistry, periodontology, prosthodontics and endodontics. He also delivers all aspects of implant treatment, from simple to complex cases. He works at Kirkgate Dental
in Tadcaster and Clarendon Dental Spa in Leeds, mainly seeing referrals
for root canal treatment and implants. Here, he discusses an endodontic case where narrow canals presented a challenge.
Initial presentation and diagnosis
The patient was a referral from his General Dental Practitioner (GDP), for root canal treatment of the lower left first molar (LL6.) The patient was 47 years old and medically fit and well. He was found to have a moderately restored dentition, with symptoms of periapical periodontitis on LL6 (see Figure 1).
The treatment options discussed were 1) root canal treatment (followed by cuspal coverage with the GDP) or, 2) extraction. As the patient was keen to save the tooth, he was keen to go ahead with root canal therapy.
Treatment pathway
Following an inferior dental and long buccal nerve block with lidocaine local anaesthetic, the old amalgam was removed in order to access the tooth. Following placement of a rubber dam, copious rinsing of the pulp chamber with buffered 5.5% hypochlorite was done.
Four root canals were located. On the distal, there was just one exit from the pulp chamber, but that quickly split into two divergent canals. The mesiolingual and mesiobuccal canals merged just at the apex. Because the canals were curved, coronal flare was needed. Also, with the canals being so narrow, long and curved, care was needed to work down the canals in order to reach the apex.
First, there was gentle scouting with a .15 C+file. This couldn’t get to the apex, in fact, it was well short. The COLTENE HyFlex™ EDM Orifice Opener 25/.12 was then used for coronal flare to a length just short of that reached by the .15 C+file. Further scouting then allowed the 15 C+file to slip further towards the apex. The Hyflex™ EDM 10/.05 Glidepath file was used next, to the distance achieved with the 015 File. Then there was scouting using a .08 C+file, getting a little bit further this time, down towards the apex. Continued work with the .08 C+file and the HyFlex™ EDM 10/.05 Glidepath file was done, until reaching the apex of each canal.
After using a rotary file, it’s useful to look to see where dentine debris is on the flutes, this shows where the file is cutting. In this case, the COLTENE HyFlex™ EDM 20/.05 preparation file was selected as the final file in the mesial canals, because dentine debris was seen on the tip of the file, demonstrating that it was the correct size for the apex.
On the distal canals, there was no dentine debris on the tip of the HyFlex™ EDM 20/.05 file. Using the HyFlex™ EDM 25/~OneFile, dentine debris was seen on the tip, so this was correct size for the distal canals. Continuous rinsing all the time during preparation with hypochlorite was done, then a penultimate rinse with 17% Ethylenediaminetetraacetic acid(EDTA)for one minute, with a final flush of hypochlorite.
All the canals were dried with HyFlex™ EDM Paper Points, and then obturated with the corresponding size-matched HyFlex™ Gutta percha Points. The Hyflex™ Gutta percha points are great in curved canals because they’re slightly stiffer than those available from other manufacturers. At this point a master point x-ray was taken.
AH+ root canal sealer was then used; and all four canals were sealed using the warm vertical condensation technique,packed down with a Buchanan
Plugger. One coat 7 universal bond, then COLTENE BRILLIANT EverGlow™Flowable composite was applied over the gutta percha, followed by COLTENE BRILLIANT EverGlow™universalcomposite.
The final X-ray showed slight sealer puffs, but these are not uncommon and will often resolve during the healing process (Figure 2).
Final outcome
The patient was happy, nicely healed and his symptoms resolved. He was returned to his GDP for cuspal coverage.
I would highly recommend the COLTENE HyFlex™ EDM file system to other practitioners. The 20/.05 file was the best choice for this kind of situation because it is narrow, strong and super-flexible for curved canals. These are difficult cases with a risk of file fracture. Even though this is mentioned to the patient pre-operatively as a warning, in my opinion COLTENE HyFlex™ EDM files greatly minimise that risk and are my files of choice for such situation
Images
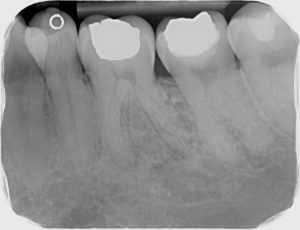
Figure 1: ll6 curved pre

Figure 2: ll6 curved post
To find out more visit www.coltene.com, email info.uk@coltene.comor call 01444 235486





